Fall Prevention & Perturbation Training, Part II: Case Studies
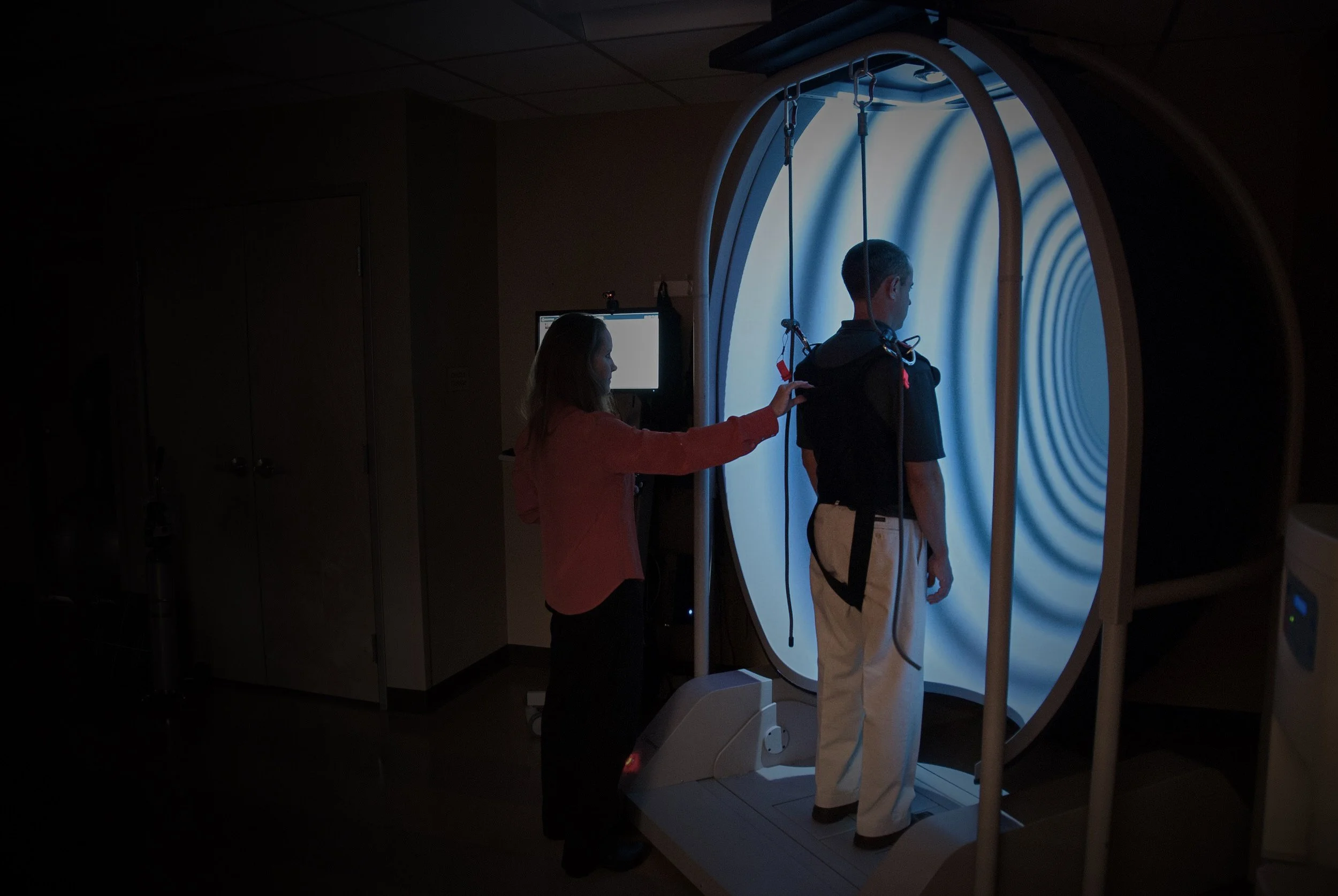
Bertec’s Immersive Labs system provides a dynamic virtual reality environment that brings perturbation training to life, allowing clinicians to safely replicate real-world fall risks while tailoring interventions to individual patient needs. Perturbation Training & Fall Prevention, Part I: Program Design provided the foundation for perturbation training.
Assessment of balance problems involves the complex interaction between many factors:
The external environment including work, home, or sport.
Multiple sensorimotor processes involved with automatic and voluntary postural control.
Biomechanical demands of maintaining the center of gravity (COG) within the limits of stability
Pathology affecting the physiological systems responsible for balance, for example Parkinson’s Disease, concussion, orthopedic injury, visual perceptual impairments, low vision, etc.
Fall risk is context-specific with each of these domains playing an important role. A thorough assessment to determine the specific impairments (e.g., sensory organization, motor control, and adaptation testing; gaze stability and dynamic visual acuity; visual motor skills; bedside examination; functional testing) is crucial in designing the most appropriate intervention program tailored to the individual’s functional goals. To illustrate the multi-factorial balance and task-specific assessments used to determine the optimal perturbation training parameters, we’ll return to the four individuals with balance problems presented in Part 1 of the Body-Brain Connection.
While exercise for health-related benefits is clear, the relationship between exercise and fall prevention is less so. Task specificity is to fall prevention intervention as intensity, frequency, duration, type, energy systems, and task are to sport and exercise prescription*. The perturbation training module allows the clinician to determine the most appropriate training parameters to match task specificity for perturbation training. The perturbation intensity is increased by increasing the challenge (randomizing perturbations, adding visual perturbations, perturbation speed and amplitude); platform movement (anterior and posterior translation, rotation); the number of perturbations in a session or the number of training sessions further determine the training volume.
The immersive virtual reality environment, unique to Bertec’s perturbation training option, permits variations in scene complexity, rotation, and movement to elicit postural adjustments. Tilting the scene left or right introduces visual conflict and evokes a head tilt response to correct subjective visual vertical, forcing the patient to reduce reliance on vision for balance. Adding force plate perturbation further increases the demands on the anticipatory and reactive automatic postural control mechanisms. For a more in-depth look at subjective visual vertical and risk of fall, look at this blog post by Dr. Charlie Shearer, O.D.
Case #1: 76-year-old grandmother with Parkinson’s Disease (PD) tripped on an uneven sidewalk, falling, and fracturing her hip. After a total hip replacement, she is currently walking with a cane. Her goal is to return to independent living in her home and participate in community activities.
Considerations: Age-related changes in vision, decreased multi-sensory processing, weakness are all factors in designing a perturbation program. Using a cane increases somatosensory input but will be a hazard if she must step to the side to recover after a perturbation. The base of support and limits of stability are restricted in those with PD: they tend to lean forward by flexing at the hips; when leaning backward, individuals take a step backward to move the base of support under the center of mass. Reactive postural responses are smaller and delayed in PD, both are factors in falls and gait disorders. Individuals with PD have difficulty with transitions between tasks and increase their external focus on the environment to maintain postural stability.
Perturbation training options: Four weeks of three sessions weekly; Begin with a low training volume; increase the number of sessions with fewer training trials and sets or total minutes to minimize fatigue. Begin with small anterior perturbations, followed by gradual progression to posterior perturbations. Post-rehab retention takes place for up to six months; consider a “booster” session at 2-6 months as has been suggested to improve retention in older adults.
Precautions: Address the emotions of anxiety and fear of falling common in those with PD; improve sense of security by using safety harness and close supervision; decrease perturbation amplitude, allowing adequate recovery time between sets; and begin with a few minutes of mindful breathing to reduce anxiety.
Case 2: 48-year-old, otherwise healthy, construction worker who tripped on an electrical cord, falling, and fracturing his wrist as he reflexively stretched out his arm to break the fall (“FOOSH” type injury).
Considerations: Assuming no other problems with multisensory processing, preventing workplace fall-related injuries requires gait adaptability (perceiving and avoiding obstacles) and the ability to react rapidly via automatic postural reactions to recover balance. Trips cause forward flexion; additional exercises to target trunk musculature and reaction time may be useful to improve trunk stability.
Perturbation training options: 2–3 sessions; focus on forward translations and add complexity with random rotation and translation, and visual scene rotation. MCT and ADT re-assessment in four weeks to assess retention.
Case 3: 36-year-old office worker who just got progressive lenses on her new glasses and slipped and fell on a wet floor.
Considerations: Address visual contributions to balance; slips cause backward extension and are more difficult to recover from; posterior perturbations best discriminate between fallers and non-fallers. The goal to rapidly develop the ability to limit trunk motion is achieved through task-specific perturbation training. Include pre- post- MCT and ADT assessments.
Perturbation training options: Consider four sessions over two weeks and monitor training reports for improvements. Follow the treatment course with a “booster” session at 2-6 months to improve retention. For slip training, a single session of high dose (challenge and repetitions) has been shown to lead to retention over 5-6 months.
A person’s function depends on the strategies one can use to increase stability to perform a given task, chiefly to maintain dynamic balance during movement. Fall risk increases with stepping, reaching, and overutilizing hip strategies to maintain balance. Task-specific perturbation training may be used as a stand-alone approach or in conjunction with conventional exercise-based approaches to significantly improve the effectiveness of fall prevention interventions (Grabiner, 2014). Bertec’s unique perturbation training module targets the semi-automatic postural responses key to fall prevention and postural control in those with neurological (post-stroke, Parkinson’s Disease, traumatic brain injury, etc.), vestibular, or orthopedic/sports (e.g., post ACL reconstruction, concussion, etc.) impairments. For more information contact [email protected].
*The exercise prescription is a specific, goal-directed plan for exercise or rehabilitation, designed by a rehabilitation specialist, based on the client’s unique needs and interests. It includes recommendations for type, intensity, frequency, and duration that are based on the specificity of training principles. The reader is referred to the ACSM Guidelines for Exercise Testing and Prescription for these evidence-based recommendations.
References
American College of Sports Medicine. (2020). ACSM's guidelines for exercise testing and prescription. 11th Ed. Lippincott Williams & Wilkins.
Cesari, P., Piscitelli, F., Pascucci, F., & Bertucco, M. (2022). Postural threat influences the coupling between anticipatory and compensatory postural adjustments in response to an external perturbation. Neuroscience, 490, 25-35.
Chmielewski, T. L., Hurd, W. J., Rudolph, K. S., Axe, M. J., & Snyder-Mackler, L. (2005). Perturbation training improves knee kinematics and reduces muscle co-contraction after complete unilateral anterior cruciate ligament rupture. Physical therapy, 85(8), 740-749.
Grabiner, M. D., Donovan, S., Bareither, M. L., Marone, J. R., Hamstra-Wright, K., Gatts, S., & Troy, K. L. (2008). Trunk kinematics and fall risk of older adults: translating biomechanical results to the clinic. Journal of Electromyography and Kinesiology, 18(2), 197-204
Hill, C. M., Wilson, S., Mouser, J. G., Donahue, P. T., & Chander, H. (2018). Motor adaptation during repeated motor control testing: Attenuated muscle activation without changes in response latencies. Journal of electromyography and kinesiology: official journal of the International Society of Electrophysiological Kinesiology, 41, 96–102. https://doi.org/10.1016/j.jelekin.2018.05.007
Horak, F. B., & Nashner, L. M. (1986). Central programming of postural movements: adaptation to altered support-surface configurations. Journal of neurophysiology, 55(6), 1369-1381.
Horak F. B. (2006). Postural orientation and equilibrium: what do we need to know about neural control of balance to prevent falls?. Age and ageing, 35 Suppl 2, ii7–ii11. https://doi.org/10.1093/ageing/afl077
Latash, M. L. (2012). Fundamentals of motor control. Academic Press.
McCrum, C., Bhatt, T. S., Gerards, M. H., Karamanidis, K., Rogers, M. W., Lord, S. R., & Okubo, Y. (2022). Perturbation-based balance training: Principles, mechanisms, and implementation in clinical practice. Frontiers in sports and active living, 4, 1015394.
Sherrington, C., Michaleff, Z. A., Fairhall, N., Paul, S. S., Tiedemann, A., Whitney, J., Cumming, R. G., Herbert, R. D., Close, J. C. T., & Lord, S. R. (2017). Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. British journal of sports medicine, 51(24), 1750–1758. https://doi.org/10.1136/bjsports-2016-096547